Biologics for COPD: A Practical Guide for Clinicians
Dr. Stephanie Christenson discusses COPD biologics, eosinophil biomarkers and trial evidence in Season 8 of The eXpand Podcast.
Sometimes the body gives no warning. No pain. No crisis. Just quiet damage unfolding over time.
Marc learned this the slow way.
Marc was 52 when he first heard the words alpha-1 antitrypsin deficiency. By then, his lungs had already lost ground he could not get back.
He had worked most of his adult life as an accountant. Long hours at a desk. Weekend hikes when time allowed. Morning jogs a few times a week. He had smoked lightly in his twenties and early thirties. A few cigarettes a day. He quit years ago and never thought of himself as a smoker in any meaningful sense.
What made his story unusual was not that he had ever smoked. It was how much lung damage he carried compared to how little he had smoked.
At first, the symptoms felt explainable. Breathlessness on hills or during jogs. A pause halfway up the stairs. He told himself it was age; he was over 50 after all. He also wondered whether those few years of light smoking were finally catching up with him. The explanation felt simple enough, so he shrugged off his symptoms and moved on, not giving it much thought.
But over time, the pattern stopped matching the story. Looking back, Marc had likely been living with gradually worsening symptoms for three to five years by this point.
Chest infections left him more short of breath than expected. Recovery took longer than it should have. Inhalers prescribed by his family doctor helped, but only a little. His lung function declined faster than his lifestyle or minimal smoking history could easily explain.
Still, the pieces were interpreted through a familiar lens.
What Marc did not know was that something fundamental was missing in his body.

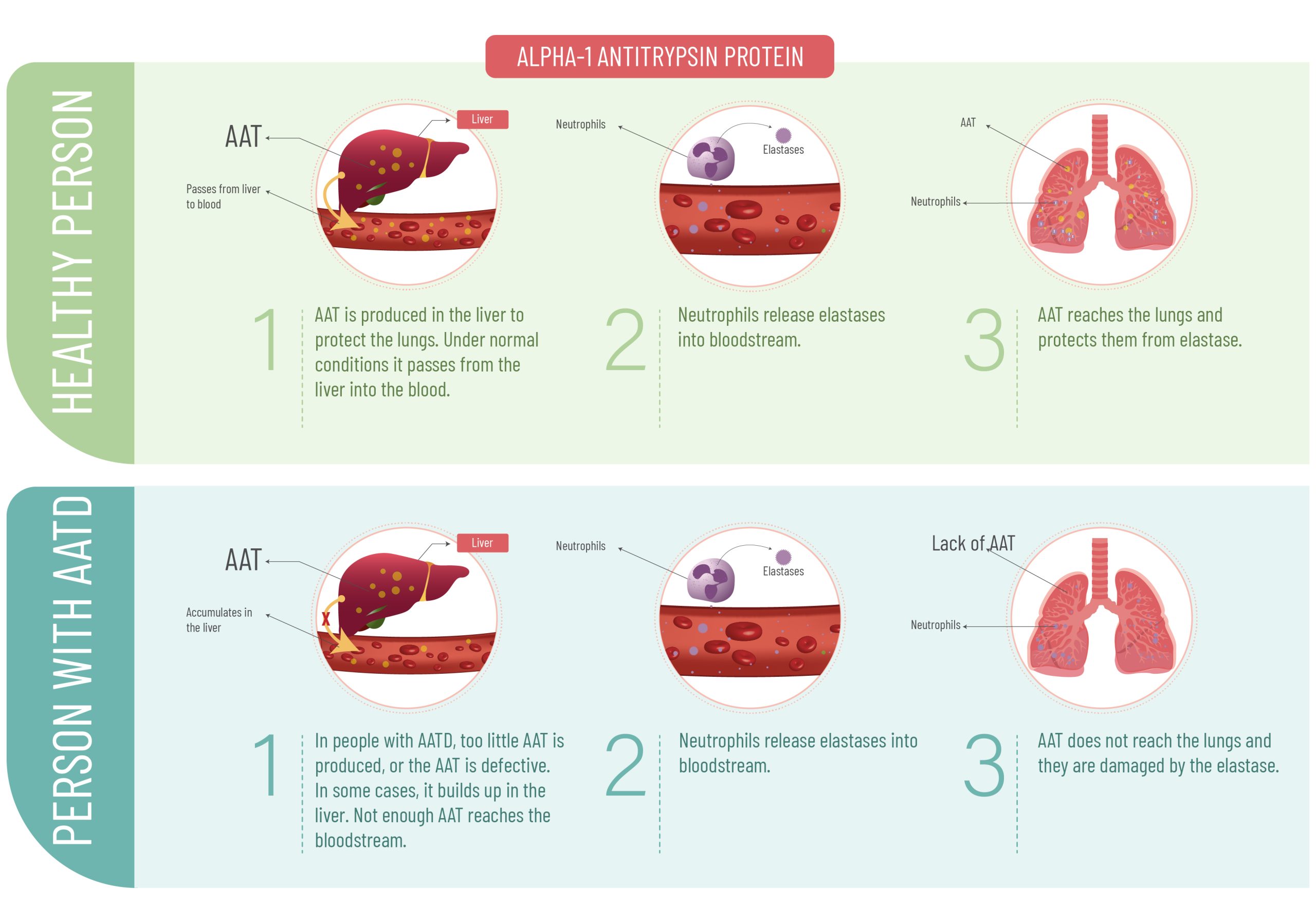
Alpha-1 antitrypsin is a protein made mainly in the liver. Its job is protective. It circulates in the blood and helps shield lung tissue from damage caused by inflammation and infection.
Every time the lungs respond to irritants, infections, or smoke exposure, alpha-1 acts as a buffer. It limits collateral damage to healthy tissue. Most people make enough of it. People with Alpha-1 do not.
In Alpha-1 antitrypsin deficiency, the body produces too little functional alpha-1 protein. In some cases, the protein is made incorrectly and becomes trapped in the liver instead of reaching the lungs. The result is the same. The lungs are left exposed and vulnerable to slow, cumulative injury.
That damage does not announce itself loudly. It accumulates over years, sometimes decades. By the time symptoms feel serious, lung function has already been lost.
That is what happened to Marc.
By the time Marc was referred to a respirologist, his lung function tests showed airflow obstruction consistent with COPD. On paper, the diagnosis fit.
What did not fit was the degree.
Given his light and remote smoking history, the extent of lung damage appeared out of proportion. The decline was faster than expected. The response to standard COPD therapy was limited. These are the moments where clinicians are taught to pause, not to assign blame, but to ask whether something else is contributing.
COPD describes a pattern of lung damage, not a single cause. Smoking is the most common contributor, but it is not the only one. In Alpha-1, the damage pattern can look similar, but the driver is genetic.
Light smoking can accelerate Alpha-1 related damage while simultaneously masking it. The exposure becomes the explanation, even when it does not fully account for the severity.
Marc’s respirologist ordered a serum alpha-1 antitrypsin level as part of a broader reassessment. It was a simple blood test. The result came back low, confirming Alpha-1.
For Marc, the diagnosis landed with mixed emotions. Relief, because there was finally an explanation. Regret, because the explanation came late. He also carried a quiet sense of guilt, which is common in people who have smoked, even lightly.
It mattered for him to hear this clearly. Smoking did not cause Alpha-1. It amplified its effects.
Alpha-1 is not rare. It is underdiagnosed. Many people live for years with lung damage attributed entirely to smoking history, even when that history is limited and remote.
The timing of diagnosis matters because Alpha-1 damage is progressive but modifiable. Once lung tissue is destroyed, it cannot be restored. But further damage can be slowed.
Early diagnosis allows for earlier referral to respirology, closer monitoring, and informed decisions about treatment, lifestyle, and infection prevention. It shifts care to focus on lung preservation, not just symptom management.
Marc’s care plan changed once Alpha-1 was identified. The focus shifted from treating presumed smoking related COPD to managing a genetic condition that required a different lens.
The diagnosis also raised a question Marc had never considered. What about his family?
Alpha-1 is inherited. That does not mean everyone in a family will be affected in the same way, or even at all. But it does mean that close relatives may carry similar genetic variants and could benefit from knowing.
These conversations require care. Genetic information carries emotional weight and concerns about confidentiality and stigma. Family testing should be offered thoughtfully, without pressure, and with clear information.
Marc chose to share the information with his siblings. One of his sisters later learned she had low alpha-1 levels but normal lung function. She now has the chance to protect her lungs early.

Alpha-1 challenges the assumption that lung damage always matches exposure. Sometimes it does not.
It reminds us that even a modest smoking history can hide a much larger biological vulnerability, and that severity out of proportion to risk factors should trigger deeper investigation.
For Marc, the diagnosis did not erase past choices. It reframed them. It replaced self blame with understanding and uncertainty with clarity.
And it reinforced a simple truth. When the damage looks bigger than the risk factors suggest, it is worth asking what else might be going on.
Alpha-1 is an inherited condition where the body has too little functional alpha-1 antitrypsin, a protective protein made mainly in the liver. This protein helps protect lung tissue from inflammation-related damage. When levels are low, lung damage can build slowly over years and cause COPD. Some people also develop liver problems because abnormal protein can build up in the liver.
Alpha-1 antitrypsin acts like a protective shield for the lungs. During infections, smoke exposure, or irritation, inflammation enzymes can damage healthy lung tissue. Alpha-1 helps keep that damage in check. Without enough functional protein, the lungs are more vulnerable to cumulative injury, which can lead to early emphysema or COPD-like changes. In some forms of Alpha-1, protein can also stress the liver.
Alpha-1 is one of the most common inherited conditions linked to COPD, but it is still underdiagnosed. It is missed because symptoms overlap with asthma and COPD, and smoking history can distract from genetic causes. Many people are diagnosed only after years of symptoms or repeated exacerbations. A simple blood serum level test can diagnose Alpha-1 earlier and change the care plan.
Yes. Smoking does not cause Alpha-1, but it can accelerate lung damage in people who have it, even with a relatively small smoking history. Some people with Alpha-1 have few or no symptoms for years, especially if they avoid smoking and reduce exposures. That is why family testing and early detection can matter: it supports prevention before major lung function is lost.
No. Alpha-1 can affect the liver because abnormal alpha-1 protein may build up in liver cells instead of being released into the bloodstream. Some people develop elevated liver enzymes, fibrosis, cirrhosis, or other liver complications. Not everyone with Alpha-1 will have liver disease, and severity varies by genetic type and other factors. Clinicians may monitor liver health as part of overall care.
Start with the simplest goal: do not miss a genetic contributor to lung damage. Alpha-1 testing is usually a serum blood level first, followed by confirmatory testing if low. Key context includes age at diagnosis, smoking or exposure history, rate of progression, and family history of lung or liver disease. These details affect how strongly results change the plan.
Many professional associations, such as the Canadian Thoracic Society, encourage testing in all people with COPD because the clinical “look” can be misleading. It is especially important in early onset COPD (often under 45 to 50), never-smokers, disproportionate emphysema, frequent exacerbations, or faster-than-expected decline. Testing once can prevent years of treating symptoms without addressing the driver.
Usually both, in sequence. The first step is commonly a serum alpha-1 antitrypsin level, a standard blood test. If the level is low (or suspicious), confirmatory testing may include phenotype or genotype testing, which clarifies the specific inherited variants. The practical point: the blood test is a simple screen, genetics helps confirm and guide family discussions.
This depends on local pathways and the severity of symptoms, but the sequence above keeps care organized and timely.
A big one is assuming smoking history rules it out. Another is skipping testing because the patient is “too old” or “does not look genetic.” Alpha-1 can present across a wide range, and environmental exposures can accelerate decline. A third mistake is stopping after a single borderline result without confirmatory testing when clinical suspicion is high.
Often, yes, but the approach should be careful and consent-based. Because Alpha-1 is inherited, first-degree relatives may want testing to understand risk and make earlier health choices. What it depends on: family planning concerns, privacy, insurance or employment worries, and emotional readiness. The best conversations are clear, non-alarmist, and centered on choice.
Not usually. A primary care clinician can often order the initial serum test as part of a COPD workup. Specialist involvement becomes most useful when levels are low, confirmatory testing is needed, symptoms are progressing, or advanced management decisions are on the table. The fastest route is often: screen in primary care, confirm and plan with respirology.
Jean Bourbeau, MD, MSc, FRCPC
Angela Diano, Executive Director, AlphaNet Canada
Katrina Metz, RT
Maria Sedeno, BEng, MM, GCSRT (Harvard)
RESPIPLUS™ received support from Takeda to develop this series specifically tailored to Alpha-1 antitrypsin deficiency (AATD).
Dr. Stephanie Christenson discusses COPD biologics, eosinophil biomarkers and trial evidence in Season 8 of The eXpand Podcast.
Explore how biologic therapies are transforming COPD care. Dr. MeiLan Han breaks down biomarkers, clinical trials, and patient selection in Season 8 of the eXpand Podcast.
Practical strategies to prevent respiratory infections in Indigenous and remote communities, including early intervention and community engagement.